

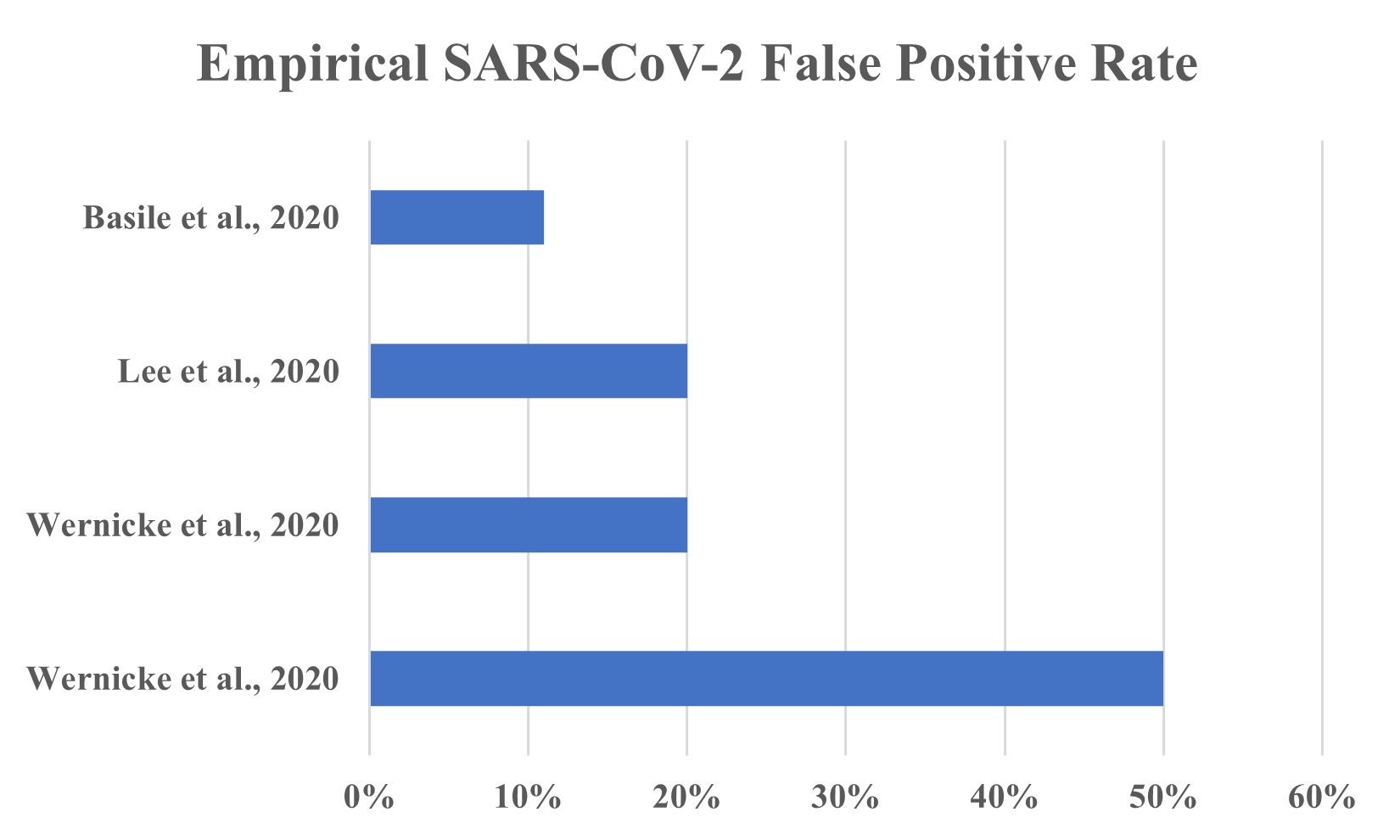
How are false reports of asymptomatic transmissions and False Positive RT-PCR test results related?? How many cases of and deaths from “COVID19” have been real? Society is depending on public health to get its facts straight on testing. Here I provide an accurate accounting of the actual state of science on the important matter of accuracy in SARS-CoV-2 testing. Here I provide the scientific literature on false positives from qRT-PCR testing, i.e.. the finding that the virus is present when it is, in fact not present. Published false positive rates are non-zero and published science-based estimates range from 11% to 50%. Claims being made that that the qRT-PCR test produces no false positive results are, sadly, woefully incorrect, reckless and irresponsible and are contributing to the decline of the ability of Americans to feed their children, pay their rent, freely associate, and to live their lives.
Quo vadis, Asymptomatic Transmission?
A study by Madewell et al. (2020) analyzed data from relevant studies to estimate the rates of transmission of SARS-CoV-2 from index (primary) cases to secondary contacts within their households. They found that index cases who were sick (symptomatic) had a household secondary attack rate (new infections attributed to the index cases) of 18%. When index cases were not sick (asymptomatic) at the time of contact, the rate of transmission to household members or relatives was only 0.7%.
One of the studies cited by Madewell et al., (2020) found that of “(t)he 299 contacts with exclusive pre-symptomatic exposures were… at risk (attack rate, 0.7% [95% CI, 0.2%-2.4%]).” In contrast, with respect to bona fide asymptomatic carriers, they state: “Among the 91 close contacts of the 9 asymptomatic cases, no secondary transmission was observed.”
A study published in Nature Communications of 9,899,828 residents of Wuhan, China found no evidence of asymptomatic transmission between May 14, 2020 and June 1, 2020 (Cao et al., 2020).
A study of transmission among US Marine recruits also shows that the virus will likely continue to transmit regardless of social distancing measures. The study, published in the New England Journal of Medicine (Letizia et al., 2020) found that in spite of masking, quarantining and social distancing, including bunking 2 by 2, recruits continuously tested positive over the duration of a 2-week training period. Of the 1848 recruits, 51 tested positive but only 5 had any symptoms prior to the positive PCR test. The number testing positive, however, also point to a possible high false positive rate: the study authors could not retrieve fully sequenceable genomes from about 37.5% of the samples from patients who had tested positive, meaning that although their test was positive, the presence of the virus may not have been a viable infection.
How can this be, when widespread testing – as recommended by public health – has the public convinced that asymptomatic transmission is common and that qRT-PCR false positives rates are “zero”?
Reports of “numbers of cases” and “numbers of deaths” can be misleading and hard to interpret out of context, especially when national public health policies and procedures on diagnostics can apparently turn on a literal dime (see, for example, New York Times, Dec 2 New York Times, CDC Now Says People Without COVID-19 Symptoms Do Not Need Testing).
They can also be made especially difficult to interpret as real risk given shifts and expected changes in the current reporting and recording standards. First, the practice of diagnosing people with COVID19 (Coronavirus Disease (20)19) was changed in April 2020, when CDC determined that it should be based on the outcome of a quantitative polymerase chain reaction test (PCR test), whether the patient has symptoms or not. The use of qRT-PCR test results alone for diagnosis of SARS-CoV-2 is fraught with problems.
Anthony Fauci’s “Dead Nucleotide Hypothesis”
The first problem is that those who do not have the disease may still test positive for the presence of viral fragments, something US NIAID’s Anthony Fauci recently referred to as “dead nucleotides”. The reference was made in the context in an interview in the podcast “This Week in Virology” (t=4:22 on the video):
Dr. Fauci: “Right again, a good question and what is now sort of, uh, evolving into a bit of a standard that if you get a cycle threshold of 35 or more that the chances of it being replication competent are minuscule so that if somebody and you know we do we have patients and it’s very frustrating for the patients as well as for the physicians somebody comes in and they repeat their pcr and it’s like 37 cycle threshold but you never if you almost never can culture virus from a 37-threshold cycle so I think if somebody does come in with 37 38 even 36 you got to say you know it’s just it’s just dead nucleotides, period. – Anthony Fauci (This Week in Virology, July 17, 2020)
The World Health Organization (Released 20/21 Jan 2021) updated the criteria for “positive for COVID19” from “one or more positive tests” to (roughly) “one or two successive positive tests and symptoms”. This means the number of tests must be doubled, but that the number of “cases” of COVID19 must decrease worldwide in nations who choose to follow their suggestion.
The State of Kansas[The Sentinel, Jan 21, 2021] has also determined that the way that PCR testing has been conducted to diagnose and count cases of COVID19 and deaths from COVID19 has been spurious and they, like the WHO, have addressed this issue and responded with policy and practice changes away from the widespread practice of allowing patients with high PCR “Cycle Threshold”, or “Ct” numbers, to be diagnosed as “COVID19”.
The widespread use of a high Ct (cycle threshold) value implies a massive bias toward reducing sensitivty of the test to zero; however, this has necessarily occurred at a cost in terms of false positives – as it would for just about any clinical diagnostic. The acknowledgement by the US NIAID, the WHO organization and the Kansas Department of Health that the use of arbitrarily high, uniform qRT-PCR cycle threshold leads to “push-through”, which then leads to unacceptably high false positive rates, will serve those who seek proof by authority.
Data, i.e., Science, exists as well. A study by Singanayagam et al (Aug 2020) showed that PCR tests results that used high Ct threshold were associated with samples that had the lowest percentage of samples that had culturable virus (5/60, or 8.3%) (their Figure 2, reproduced below). These made up only 1.5% of all culture positive samples in the study.

Given how clinical, CLIA-certified qRT-PCR experiments are conducted, there is no scientific basis for a “standard Ct threshold”. First, all tests have their own optimization – indeed, each primer pair in each test will have their own optimization. Each run for each patient should include data from the patient’s sample – and data from a buffer solution that serves as a negative control. The buffer should be free to the target sequences and serves as a negative control. Each patients’ assessment should be based on the differences in the Ct values between the buffer and the patient (a measure called;” Delta-Ct”, or DCt). It is the relative difference between the patient and the control sample that would determine if a qRT-PCR test is positive or negative, not the solitary absolute measure of Ct from a patient.
In addition to Anthony Fauci’s dead nucleotide hypothesis, a person may have a preliminary superficial infection that is going to resolve because they are already immune.
Further, the test kits themselves have intrinsic false positive rates – characteristic of the test kits. These should have been reported to the FDA in the Emergency Use Authorization filing. EUAs for tests, however, were initially given out without requiring empirical estimates of the false positive rates. Instead, the FDA allow companies to predict whether their kits would yield false positives based on a purely computational exercise called BLAST: the nucleotide sequences used in the primers in their PCR kits were compared to the human genome, and if no significant matches were found, it was assumed that there could be no false positive results. We now know that that assumption was incorrect.
False Positives Are Not Zero
Contrary to widespread claims made by public health departments and commercial kit makers, the empirical specificity of qRT-PCR has, unfortunately, not proven to be 100%. In fact, it never could have. Basile et al. (2020) reported a FPR of 11%. Lee (2020) reported a FPR of 20% in a collection of 20 reference samples. A study of Marine recruits could not generate a full SARS-CoV-19 genome in 37.3% of PCR-positive recruit samples (Letizia et al. 2020) and recalling the review that found false positive rates ranging from 20-50% (Wernike et al., 2020), the science shows that Departments and Boards of Health are badly misinformed.
False negatives are also a concern. A study by Peñarrubia et al. (2020) found that 8.5% of all mutations (new nucleotide differences) in SARS-CoV-2 variants around the world map to known PCR primer locations. These locations make up far less than 8.5% of the 29K nucleotide base viral genome; hence, we can be certain that variants that have escaped the test are circulating and will increase in frequency unless the problems and limitations with the current qRT-PCR – based diagnosis protocol are addressed. Otherwise, it is inevitable that SARS-CoV-2 will spread due to test escape leading to false negatives (missed, new test-escape variants) at an increasing rate no matter what anyone does.
What Can and Should be Done
To deal with false positives, Peñarrubia et al. (2020) suggest using more than one qRT-PCR test type per patient to avoid false positives, however, that paradigm will also fail due to the incessant force of evolution, and we need tests that are robust to evolutionary pressures and that are 100% specific (zero false positives). Dao et al (2021) 2.4 to 69.2% of patients hospitalized for COVID19 could still test positive 1 to 38 days after being discharged – and they had no explanation why. They also suggested using multiple test types per patient and sampling from different parts of the body. Such ad-hoc solutions are likely to decay the reproducibility and reliability of testing while greatly increasing the cost and complexity.
As late as July 2020, Dr. Redfield of the CDC told CNN Correspondent Sanjay Gupta that the US needed a viable COVID19 testing strategy. Nothing has changed since July. As a result these failures, testing paradigms have been modified to include repeat testing via the same or different PCR tests a few days later. This window of testing leads to delay, additional cost, and can result in disparate test results in the same patient. The result is a shift to diagnose every respiratory illness case – test result or no – as COVID19 (suspected or “confirmed”). The absence of influenza diagnosis is further evidence of this fact. False positives mean that “confirmed” does not mean confirmed. The reality is that the testing paradigm that has emerged is one in which individuals with one, or two, or even zero positive PCR test results are given a positive COVID19 diagnosis, leading (necessarily) to inaccurate reports in the number of cases and numbers of death (Ealy et al., 2020). False positive results can have serious clinical consequences ranging from inappropriate treatment of respiratory illnesses (e.g., bacterial pneumonia misdiagnosed as “COVID19”) and delays in emergency surgery (Katz et al., 2020) and misattribution of cause of death.
PCR Test Escape Variants Detected – And More Expected
Evidence suggests that widespread qRT-PCR testing alone – without sequencing – has led to – and will continue to lead to – test escape by new variants. The UK variant (202012/01 aka B.1.1.7, 20I/501Y.V1) which is widely considered to be “more transmissible” has seven variants in the nucleotide sequences encoding the spike protein; one of the primers in the spike region fails with the UK variant. Before this was discovered, the UK variant diagnosis was likely 50% less sensitive due to the S-gene dropout because the algorithm for the test requires ⅔ of primers pairs to each successfully amplify its target amplicon. The role of escape of the test for the UK variant contributing to its spread until the testing algorithm allowed 2/2 positive primer pairs results instead of the original ⅔ is certain. Further, a study found that 8.5% of all known mutations among SARS-CoV2 variants were located in known qRT-PCR primer sites, leading the authors to suggest the use of two different qRT-PCR assays per patient, which is untenable, complex, expensive and wasteful.
This entire debacle began when CDC shipped flawed tests in March 2020. Ask any competent laboratory technician or molecular pathologist: PCR tests by themselves cannot be gold-standard clinical test; the FDA gold-standard for the validation of PCR tests is Sanger nucleotide sequencing (FDA, 2020). This technique was used by Lee (2020) to determine that a reference sample set not only included 20% false positives, but also 30% false negatives.
To resolve ambiguities in testing, I recommend whole genome sequencing, allowing simultaneous and comprehensive diagnosis of suspected pathogens, including influenza A and B, respiratory syncytial virus, and others, including the SARS-CoV-2 virus. While costly, the cost of the current unvalidated testing paradigm to society has been too much (Lyons-Weiler, 2020a). it is time to rethink public health from the ground up and abandon appeals to authority as singular viable sources of information on reality (Lyons-Weiler, 2020b).
The practice of automatically determining that people who have died with a positive PCR test, or a presumed diagnosis of COVID19 without a PCR test, was determined by a unilateral decision by the CDC who made the decision to change medical practice and death reporting without going through proper channels as required by law (Ealy et al., 2020), which would have provided proper review of the potential consequences of public health unilaterally dictating medical standards of care across the country. It is my opinion that this decision and favoring false positives over false negatives in PCR tests, will ultimately be determined to have helped contribute to the loss of hundreds of thousands of small businesses, lockdowns, school closures, hunger, and deaths of despair including a shocking increase in suicides among teens (Lyons-Weiler, 2020).
These issues are central and of utmost importance to the issues of the case because the number of cases can become greatly exaggerated by an errant testing protocol, and the number of deaths “from COVID” exaggerated by the reporting criteria. This bias is having a devastating effect on society. Listen to Dr. Scott Jensen as he makes a plea to his colleagues to de-legitimize medicine via audits on causes of deaths:
Boards and Departments of Health should be able to produce key data that show that the numbers of cases and deaths reported for a state or region are accurate. Specifically, they should be able to produce data on the false positive rate of the process of diagnosing and reporting “COVID19” given the protocols in use around a given county or State.
Boards and Departments of Health should also be able to produce data on the positivity of tests and numbers of tests for influenza viral infection-related deaths (not the general categorial “influenza disease” or “pneumonia & influenza”) and other COVID19-like illnesses, such as bacterial pneumonia. Departments of Health should be able to produce estimates of the infection case fatality rate (ICFR – the death rate in confirmed infections) overall and by age for a county, region or state.
Boards and Departments of Health should be able to provide data on how many and what percentage of cases had comorbid conditions.
Boards and Departments of Health should have reported and should now report data on the number of people who died from COVID19 who were already frail or infirm; the number who were residents in nursing homes, or in hospice.
Boards and Departments of Health should be able to produce data showing how many “COVID19” cases and deaths are “presumed COVID19” without a positive PCR test, and how many “COVID19” cases and deaths are likely to be non-COVID respiratory illnesses.
Boards and Departments of Health should be able to provide a timeline (complete provenance) of the practices and procedure from January 2020 to the present day on policies and practice standards for data capture and reporting should be provided, along with correspondences to and from the US Centers for Disease Control and the US Department of Health and Human Services related to procedures and updates to procedures for data reporting.
Clinical Sequencing is Part of the Solution
Changing the criteria of “died with” vs. “died from” back to pre-April 2020 practices is necessary.
If the reporting and recording criteria for COVID19 “cases” are not biologically and medically accurate, no rational basis for a public health policy around COVID19 exists. If the CDC and Department of Health around the country also concede – or decide themselves – as many suspect they soon will – that the use of high Ct numbers have exacted an unnecessary and unsustainable burden on society in terms of quarantining and isolating people who do not have to be isolated, shutting businesses that do not have to be shut down, or placing demands on the details of how businesses conduct themselves, the number of COVID19 cases will plummet, falling below the threshold for the State of Emergency. The outcome could be a revelation that the high Ct threshold used in the past was damaging to society without reason.
Whatever is done, the most important fact that must be accepted is that empirical field estimates of the false positive rates of qRT-PCR tests used to detect SARS-CoV-2 are non-zero. When the prevalence of an infection in the population is low, over-testing will result in far more false positive test results than true positive – and yet the false positive results are still counted, per CDC’s decision in April, as “cases”. Understanding the link between the positive and negative predictive value of a test and prevalence is essential to understanding why false positive matter so much. From Wernicke et al. (2020):
Dr. Sin Hang Lee’s study concluded that FDA Gold Standard validation of PCR testing should be conducted. In my view, sequencing to know which pathogen (if any) is truly present in the symptomatic and in the exposed only is the singular scientifically defensible position that anyone in molecular diagnostics should adopt. Sequencing the amplicon (the product of the PCR reaction) will lead to 0% false positives, however, care must be taken to ensure that nested primer sets are utilized in case the SARS-CoV-2 viral lineages escape the test due to mutations in the primer locations.
“If we assume a best-case scenario for specificity based on these results for the A-3 or B/E-Sarbeco setting, the diagnostic specificity was calculated as 0.9756 (40/41; Table 1). In calendar week 14 of 2020, 36,885 out of 408,348 samples (9.0%) tested positive in Germany (Robert-Koch-Institut, 2020). Under these conditions, the positive predictive value of the test system was 0.802, that is almost 20% of the positive results would have been false-positive. In calendar week 19, 10,187 out of 382,154 samples (2.7%) tested positive. In this scenario, a test system with a diagnostic specificitty(sic) of 0.9756 had resulted in a positive predictive value of 0.5319, that is almost half of the positive results would have been false-positive. Obviously, any further reduction of the prevalence of SARS-CoV-2 infections will result in decrease of the positive predictive value if the specificity of the employed assays is not dramatically increased.”
The American Association for Clinical Chemistry published an article on false positives from PCR testing for SARS-CoV-2 in October, 2020. The author distinguishes between symptom-based/exposure-based testing vs. screening and points out that existing validation steps are not used to confirm the qRT-PCR results.
The paired decisions by CDC and public health in general to use qRT-PCR testing alone, without sequencing, and to conduct the tests in a manner that favors test sensitivity over test specificity was unnecessary and has unquestionably led to an overestimation of the number of cases and deaths due to COVID19 everywhere. Boards of Health should be able to provide data estimating the FPR in a case audit and revise their case and death counts to date so a rational position on the actual risk of exposure and risk of death from COVID19 infection can be ascertained and considered by the public, the legal system and the medical community.
Over-counting cases, even if done out of an abundance of caution, externalizes the cost of inexact testing to the rest of society is ways that can be profoundly costly. The actual cost depends on the overall cost of the false positive to society and the cost of the false negative (Lyons-Weiler, 2020). Knowing these costs has far more impact on total cost to society than “more testing” or “less testing”.
Science shows that the false positive rate of SARS-CoV-2 PCR tests is not “zero”. It is time for the United States to choose between public health and medical practices based on Science, and those based on the fallacy of appeal to authority, which have so repeatedly and badly failed us. When public health fails to follow the science, we all pay dearly. We need Plan B (Lyons-Weiler, 2020b).
References
Basile K, Maddocks S, Kok J, Dwyer DE. Accuracy amidst ambiguity: false positive SARS-CoV-2 nucleic acid tests when COVID-19 prevalence is low. Pathology. 2020 Dec;52(7):809-811. doi: 10.1016/j.pathol.2020.09.009. Epub 2020 Sep 30. PMID: 33087255; PMCID: PMC7524665.
https://pubmed.ncbi.nlm.nih.gov/33087255/
Cao S, Gan Y, Wang C, Bachmann M, Wei S, Gong J, Huang Y, Wang T, Li L, Lu K, Jiang H, Gong Y, Xu H, Shen X, Tian Q, Lv C, Song F, Yin X, Lu Z. Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China. Nat Commun. 2020 Nov 20;11(1):5917. doi: 10.1038/s41467-020-19802-w. PMID: 33219229; PMCID: PMC7679396.
Dao TL, Hoang VT, Gautret P. Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: a narrative review. Eur J Clin Microbiol Infect Dis. 2021 Jan;40(1):13-25. doi: 10.1007/s10096-020-04088-z. Epub 2020 Oct 28. PMID: 33113040; PMCID: PMC7592450. https://pubmed.ncbi.nlm.nih.gov/33113040/
Ealy, H, M McEvoy, D Chong, J Nowicki, M Sava, S Gupta, D White, J Jordan, D Simon and P Anderson. COVID-19 Data Collection, Comorbidity & Federal Law: A Historical Retrospective. Science, Public Health Policy & the Law Oct 2020 2:4-22.
Katz AP, Civantos FJ, Sargi Z, Leibowitz JM, Nicolli EA, Weed D, Moskovitz AE, Civantos AM, Andrews DM, Martinez O, Thomas GR. False-positive reverse transcriptase polymerase chain reaction screening for SARS-CoV-2 in the setting of urgent head and neck surgery and otolaryngologic emergencies during the pandemic: Clinical implications. Head Neck. 2020 Jul;42(7):1621-1628. doi: 10.1002/hed.26317. Epub 2020 Jun 12. PMID: 32530131; PMCID: PMC7307014.
Letizia AG, Ramos I, Obla A, Goforth C, Weir DL, Ge Y, Bamman MM, Dutta J, Ellis E, Estrella L, George MC, Gonzalez-Reiche AS, Graham WD, van de Guchte A, Gutierrez R, Jones F, Kalomoiri A, Lizewski R, Lizewski S, Marayag J, Marjanovic N, Millar EV, Nair VD, Nudelman G, Nunez E, Pike BL, Porter C, Regeimbal J, Rirak S, Santa Ana E, Sealfon RSG, Sebra R, Simons MP, Soares-Schanoski A, Sugiharto V, Termini M, Vangeti S, Williams C, Troyanskaya OG, van Bakel H, Sealfon SC. SARS-CoV-2 Transmission among Marine Recruits during Quarantine. N Engl J Med. 2020 Dec 17;383(25):2407-2416. doi: 10.1056/NEJMoa2029717. Epub 2020 Nov 11. PMID: 33176093; PMCID: PMC7675690.
Lee, SH. 2020. Testing for SARS-CoV-2 in cellular components by routine nested RT-PCR followed by DNA sequencing International Journal of Geriatrics and Rehabilitation 2(1) 69-96.
Lyons-Weiler, 2020a. Balance of Risk in COVID-19 Reveals the extreme cost of the false positives. Intern J Vacc Theor, Pract, Research 1(2):209-222.
Lyons-Weiler, J. 2020. Lyons-Weiler, J. 2020b. Plan B public health infrastructure and operations oversight reform for America. Intl J Vacc Theor, Pract, Research 1(2):283-294.
Madewell ZJ, Yang Y, Longini IM Jr, Halloran ME, Dean NE. Household Transmission of SARS-CoV-2: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020 Dec 1;3(12):e2031756. doi: 10.1001/jamanetworkopen.2020.31756. PMID: 33315116; PMCID: PMC7737089. https://pubmed.ncbi.nlm.nih.gov/33315116/
Peñarrubia L, Ruiz M, Porco R, Rao SN, Juanola-Falgarona M, Manissero D, López-Fontanals M, Pareja J. Multiple assays in a real-time RT-PCR SARS-CoV-2 panel can mitigate the risk of loss of sensitivity by new genomic variants during the COVID-19 outbreak. Int J Infect Dis. 2020 Aug;97:225-229. doi: 10.1016/j.ijid.2020.06.027. Epub 2020 Jun 12. PMID: 32535302; PMCID: PMC7289722.
US Food and Drug Administration. Memorandum. Guidelines for the Validation of Analytical Methods for Nucleic Acid Sequence-Based Analysis of Food, Feed, Cosmetics and Veterinary Products. Accessed 1/30/2021 https://www.fda.gov/media/121751/download
US Food and Drug Administration Emergency Use Authorization (EUA) information, and list of all current EUAs. https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and-policy-framework/emergency-use-authorization
Wernike K, Keller M, Conraths FJ, Mettenleiter TC, Groschup MH, Beer M. Pitfalls in SARS-CoV-2 PCR diagnostics. Transbound Emerg Dis. 2020 Jun 14:10.1111/tbed.13684. doi: 10.1111/tbed.13684. Epub ahead of print. PMID: 32536002; PMCID: PMC7323359

Thank you very much, Dr. Lyons-Weiler.
World Health Organization Warns of ‘False Positives’ in PCR Tests for Covid-19, Says Some Patients May Not Be ‘Truly Infected’
https://needtoknow.news/2021/02/world-health-organization-warns-of-false-positives-in-pcr-tests-for-covid-19-says-some-patients-may-not-be-truly-infected/?utm_source=rss&utm_medium=rss&utm_campaign=world-health-organization-warns-of-false-positives-in-pcr-tests-for-covid-19-says-some-patients-may-not-be-truly-infected
I have a comment & a question (neither directly related to this post; sorry.)
1) Comment: I watched your interview on the tribunal panel with OCA and appreciated everything you had to say, as usual. With regard to fighting for freedom of speech, one of the things I’ve noticed is that health departments across the country are making bold statements on their websites without providing any citations to back them up. I’ve even seen official government health department websites post hard numbers for the supposed effectiveness of masks — with zero hint as to where those numbers came from.
One major action point is that I think people need to start pushing back on this. Contact their health departments and ask them, “what is the evidence for that statement?” I sent an email last week to my state health department asking them to please provide the evidence behind their claims that Covid vaccinations will protect our teens, that they’ll be guaranteed unable to spread it after vaccination, etc. People need to be doing this all over the country — force the people WE’RE paying to give us science-based recommendations to demonstrate that their recommendations are based on science.
2) Question: Prominent doctors have recently determined that several of the new variants are more infectious because of a modification in their spike protein that stabilizes the protein by preventing it from folding in on itself. They say this enables a larger percentage of the spike proteins to persist. (I’m paraphrasing all this; I can provide a link if necessary but I’m not sure if your comments allow links.) As I understand it, the spike protein in the Moderna and/or Pfizer products (I’m not 100% sure if it’s both) is modified to stabilize it by preventing it from folding in on itself. What needs to be done to determine whether the vaccine-modified spike protein is showing up in these variants or whether these are just separate modifications that coincidentally have the same effect?