Article Text

Abstract
Objective Persistent exposure to faecal pathogens due to open defecation may cause environmental enteropathy that, in turn, may lead to undernutrition and vaccine failure in under 5-year-old (u5) children. The Swachh Bharat Mission (SBM) programme in India, launched in 2014, aimed to construct toilets for every household nationwide and reduce open defecation. This programme, if successful, had the potential to reduce the burden of four vaccine preventable diseases (VPDs): diphtheria, pertussis, tetanus and measles. We examine whether increased household toilet availability in Indian districts following SBM corresponds with a reduction in diphtheria, pertussis, tetanus and measles in u5 children.
Design Observational, ecological study.
Setting 532 districts in 28 Indian states, from 2013 to 2016.
Primary outcome and exposure We retrieved data on district-level change in the annual incidence (per 1000 u5 children) of four VPDs, from 2013 (pre-SBM) to 2016 (post-SBM). We obtained data on our exposure, the change in the percentage of households with toilets (per district), from three large national surveys conducted in 2013 and 2016. We used linear regression analysis, which controlled for change over time in socioeconomic factors, health system-related covariates and pre-SBM annual incidence of VPDs.
Results A one percentage point increase in households with toilets corresponds with 0.33 fewer measle cases per 1000 u5 children in a district (coefficient: −0.33, 95% CI −0.0641 to –0.014; p<0.05). About 12% of this association is mediated by a reduction in u5 stunting. We observe no relation of the exposure with diphtheria, pertussis or tetanus. Findings remain robust to sensitivity analyses.
Conclusion Rapid improvements in ambient sanitation through increased toilet availability correspond with a reduction in the annual incidence of measles in u5 children. We encourage replication of findings and further research to identify potential pathways by which SBM may reduce measle burden in u5 children.
- public health
- community child health
- paediatric infectious disease & immunisation
- public health
- social medicine
- epidemiology
Data availability statement
Data are available in a public, open access repository. The datasets underlying this article are available from the following sources in the public domain: 1. Health Management Information System (HMIS) India: Health Management Information System: A digital initiative under National Health Mission. Ministry of Health & Family Welfare, Government of India. 2020. Available from: https://dhsprogram.com/pubs/pdf/FR339/FR339.pdf 2. Annual Health Survey (second round): Annual Health Survey (AHS) India. Office of the Registrar General and Census Commissioner (India) 2014. URL: http://www.censusindia.gov.in/2011census/hh-series/cab.html 3. District Level Household and Facility Survey (DLHS-4), 2012–13. IIPS, International Institute of Population Sciences, Mumbai, India. Deonar, Mumbai, 2014. URL: http://www.nrhmmis.nic.in/SitePages/DLHS-4.aspx 4. National Family Health Survey (NFHS-4): International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey (NFHS-4), 2015-16: India. Mumbai: IIPS 2017. URL: https://dhsprogram.com/pubs/pdf/FR339/FR339.pdf.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- public health
- community child health
- paediatric infectious disease & immunisation
- public health
- social medicine
- epidemiology
Strengths and limitations of this study
Strengths include our use of nationally representative survey and administrative data spanning nearly all districts in India for longitudinal analysis of changes in annual incidence of vaccine preventable diseases (VPDs) in relation to percentage of households with toilets from 2013 to 2016.
Limitations include that we do not examine the relation between VPDs and district-level availability of household toilets by rural or urban regions and by child gender (male, female) owing to lack of data availability by these subgroups.
Limitations also include non-examination of shared toilets owing to lack of household-level VPD data.
Introduction
In 2019, India recorded the highest number of diphtheria and tetanus of any country worldwide.1 India also ranked among the top 10 countries worldwide in pertussis and measle cases.1 Between 2000 and 2020, the annual incidence of these diseases under 5-year-old (u5) children in India averaged 32.8 for measles, 3.5 for diphtheria, 31.1 for pertussis and 3.3 for tetanus per 100 000 population.1 In 2010, measles accounted for about 3% of all u5 deaths in India.1 2 Tetanus accounted for approximately 20 deaths per million live births during the same time period,3 contrasting sharply with other low and middle-income countries that exhibit substantially lower u5 mortality from vaccine preventable diseases (VPDs) relative to India2. Whereas overall cases for these VPDs declined steadily over the past decade, India’s abysmal global ranking raises questions about low vaccine effectiveness despite its nearly 80% immunisation coverage following the initiation of the Universal Immunization Program in 2012.4
Improved sanitation in a community may play a role in strengthening children’s immune response.5 Owing to lack of toilets and the widespread practice of open defecation, India serves as a unique case study.6 7 Over 60% of the global population that practices open defecation lives in India.6 7 Prolonged exposure to faecal pathogens may cause environmental enteropathy.8 This condition, or syndrome, includes nutrient malabsorption in the small intestine, atrophy of intestinal villi, crypt hyperplasia, T-cell infiltration and inflammation of the jejunum.5 8 Environmental enteropathy may cause undernutrition that, in turn, may lead to immune dysfunction and impairment.5 Researchers assert that levels of antibodies produced after vaccination are lower among malnourished children and that environmental enteropathy contributes to this phenomenon.9 Moreover, environmental enteropathy can diminish vaccine-specific responses10 11. Whereas environmental enteropathy is better characterised with respect to oral vaccine responses10 11 (eg, polio and rotavirus), although with mixed evidence,12 13 studies also find an association between enteropathy and diminished parenteral vaccine response through suppressed immunity, altered gut microbiota and undernutrition.14–16 Researchers have reported such associations for measles, diphtheria, pertussis and tetanus (DPT), especially among undernourished u5 children.9 17–19
Environmental enteropathy poses a key risk to child development starting from a very early age (first 1000 days of life).20–25 Encouragingly, rapid improvements in ambient sanitation may reverse environmental enteropathy within a relatively short time span.26 27 In October 2014, the Indian federal government launched one of the world’s biggest national sanitation programmes—the Swachh Bharat Mission (SBM). SBM aimed to construct toilets for every Indian household and eliminate the practice of open defecation by 2019.28 Over this 5-year period, the SBM programme received annual funding of over $1 billion. Over 100 million toilets have been constructed across the country by 2019.28 This programme combined financial incentives for toilet construction (at the household level) with intensive behavioural change messaging through multiple channels (eg, community mobilisation, social media, radio, television, public service announcements and cinema) that promoted toilet utilisation and sanitary behaviours. Whereas India has implemented other sanitation policies in the decades preceding SBM, none of the prior programmes combined public awareness campaigns with toilet construction on the scale of SBM.29
Recent work suggests that increased toilet availability following SBM may have reduced child undernutrition30 and diarrheal outbreaks.31 However, we know of no work that examines whether these improvements extend to reduced annual incidence of VPDs among u5 children. We leverage the quasi-random nature of the SBM programme to examine whether large increases in toilet availability correspond with reductions in each of four VPDs in u5 children- diphtheria, pertussis, tetanus and measles. Given that the timing and national scale of SBM was not determined by local district-level decisions, the study design confers three main strengths. First, a ‘common cause’ is not likely to drive both VPDs and the SBM campaign. Second, the exposure (SBM) precedes the outcome and thereby establishes temporal order. Third, SBM is not ‘caused’ by district-level variations in the VPDs. These attributes reduce inferential threats from selection bias and potential reverse causation.
Methods
Data and variables
Starting in 2012, the Government of India’s National Health Mission publishes annual district-level data on the annual incidence of VPDs among u5 children through a Health Management Information System (HMIS) portal.32 While its relative novelty has precluded it from wide use, recent literature acknowledges the superiority of HMIS data over previously existing databases on immunisation and VPDs in India.33 34 The HMIS reports annual district-level information on immunisation, adverse events and annual incidence of DPT, measles and other illnesses among u5 children.32 These data serve as a central repository of VPD surveillance across India and undergo several rounds of validation checks at village, subcentre, block, district and state levels.35 HMIS data files are publicly available.32 We used these data to retrieve information on our outcomes of interest: the change in annual incidence of (a) diphtheria (b) pertussis (c) tetanus and (d) measles per 1000 u5 children, per district, from 2013 (pre-SBM) to 2016 (post-SBM), for all Indian districts.
We retrieved data on our exposure (district-level change from 2013 to 2016 in percentage of households with toilets) from three national survey data sets. These three data sets comprise (a) District Level Household & Facility Survey, round 4 (DLHS-4), (b) Annual Health Survey (AHS, second update) and (c) National Family Health Survey, round 4 (NFHS-4). DLHS-4 is a nationwide survey sponsored by the Ministry of Health and Family Welfare and covers 21 states and union territories (321 districts) with 1000 to 1500 households sampled under each district.36 AHS is sponsored by the Office of the Registrar General, India, on behalf of the Ministry of Health & Family Welfare for nine high-risk states that have traditionally fared the worst in terms of child health indicators in India.37 AHS covers 284 districts with an average of 12 000 households sampled per district.37 The DLHS-4 and AHS data sets report information for 2013 (pre-SBM). The NFHS is a decennial survey in India administered through the Demographic Health Surveys Program and its fourth round (NFHS-4) reports data for 2016 (post-SBM).38 Its sample size is approximately 572 000 households, in 640 districts across all 29 states and 9 union territories in India.38 NFHS-4, unlike its predecessor (NFHS-3), contains substate geographic identifiers, permitting the use of districts as the unit of analysis.38 Households surveyed in DLHS-4, AHS and NFHS-4 are sampled to be representative (in aggregate) at the district level and have been used extensively in pooled longitudinal format.39 40 According to an analysis by the WHO, these data sets have been used in over 600 scientific publications, in addition to extensive utilisation by the World Bank, Government of India and other policy making agencies.41
The HMIS data report the relative percentage of VPDs to total reported childhood diseases (per district, per year). We converted these percentages to annual incidence of VPDs by following a two-step process. First, we used the number of u5 children reporting by illness from the AHS, DLHS and NFHS data sets to get the count of u5 children reporting VPDs. Next, we used the population-weighted survey data sets (AHS, DLHS and NFHS) to obtain the counts of u5 children per district, per year. This district-level count of u5 child population was used as the denominator, with the number of u5 children reporting VPDs (estimated in the first step) as the numerator, multiplied by 1000, which yielded our outcome variable. Using these survey data sets, we also calculated the number of households reporting use of unshared (ie, personal) toilets as a percentage of total number of surveyed households per district in 2013 and 2016. We defined our exposure as the difference in district-level percentage of households with toilets in 2016 relative to 2013. We also obtained a set of control variables from the DLHS-4, AHS and NFHS-4 data sets to account for factors that may have changed from 2013 to 2016 and that might be associated with changes in Annual incidence of VPD. These variables include change in percentage of households with electricity, percentage of households with clean drinking water (boiled and/or treated), percentage of households with clean cooking fuel (liquefied petroleum gas and/or biogas), percentage of women with 10th grade or higher education, percentage of child births in hospitals (institutional deliveries), percentage of ≤1-year-old children who received DPT vaccine and percentage of ≤ 1-year-old children who received the measle vaccine. A large literature describes the role of these variables in determining child health outcomes in developing countries.42 Their inclusion reduces confounding by general improvements in district-level health systems and socioeconomic attributes that may cooccur with implementation of the SBM programme over the study period. Our final analytic file containing districts reported uniformly across all data sets (HMIS, DLHS-4/AHS, NFHS-4) comprised 532 districts as the units of analysis. Gujarat, Jammu & Kashmir and a few Union Territories were excluded as they were not covered in the pre-SBM survey data sets (AHS, DLHS-4).
Analysis
We specified the following test equation:
 ΔPercentage of households with toilets +
ΔPercentage of households with toilets +  Baseline annual incidence of VPD +
Baseline annual incidence of VPD +  ΔControls + ε (Equation 1)
ΔControls + ε (Equation 1)
where
 is the change in annual incidence of VPD (2016 minus 2013) per 1000 u5 children per district, examined separately by VPD type (DPT and measles).
is the change in annual incidence of VPD (2016 minus 2013) per 1000 u5 children per district, examined separately by VPD type (DPT and measles).
ΔPercentage of households with toilets is the change in percentage of households with toilets (2016 minus 2013) per district.  serves as the main coefficient of interest.
serves as the main coefficient of interest.
Baseline annual incidence of VPD is the pre-SBM (ie, 2013) annual incidence of respective VPD per 1000 u5 children.
ΔControls is the vector of control variables (2016 minus 2013) listed earlier.
εis the heteroscedasticity-robust SE term.
We used ordinary least square regression analysis to estimate equation 1 separately for each VPD. For tests that rejected the null, we stratified equation 1 by India’s administrative regions (central, eastern, northern, north eastern, southern and western) to explore which regions show the greatest change in outcome per increase in exposure. In addition, for any results which rejected the null, we then reformulated the outcome as change in counts (as opposed to per 1000 annual incidence) of VPDs in u5 children per district to obtain the average marginal effect of change in exposure on the outcome (case counts). We also conducted exploratory analyses of mediation (child undernutrition modelled as stunting among u5 children)30 and sensitivity to additional covariates that may influence VPDs that exhibit statistically detectable associations with the exposure. Finally, for tests that rejected the null, we conducted robustness checks to examine whether our analytic results and inference were influenced by outliers. For all analyses, we specified robust SEs (clustered by state) to account for correlated errors to account for within-state correlation (ie, spatial ‘clustering’). We conducted all analyses in Stata SE V.14.2.43
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Results
Table 1 describes the mean and SD of the covariates included in our study by pre-SBM and post-SBM as well as the change over this period. The annual incidence of VPDs in u5 children (per 1000) declines from 2013 to 2016. Measles shows the greatest reduction, followed by DPT. These trends align with India’s national surveillance data reported by the WHO.44 Mean percentage of households with toilets per district increases from 45% in 2013 to 53% in 2016, which agrees with other reports.45 Online supplemental appendix table 1 describes the distribution of outcome variables (mean) at various percentiles. Most districts (from the 25th to 95th percentile) report no change from 2013 to 2016 in DPT, except at the lowest (first to 10th) and highest (95th to 99th) percentiles of change. The distribution of change in annual incidence of measles (per 1000 u5 children) over time is relatively more uniform across all percentiles of change.
Supplemental material
Mean and Standard Deviation (SD) of variables pre-SBM (in 2013), post-SBM (in 2016) and change over time (post-SBM − pre-SBM) across 532 districts (28 states) in India
Figure 1 maps the district-level change in VPDs (2016 minus 2013) across India. Sections of Gujarat, Jammu & Kashmir, Bihar, Maharashtra, Madhya Pradesh and Telangana show reduction in diphtheria (figure 1A). Annual incidence of pertussis does not change in most regions (figure 1B). Tetanus in u5 children declines in some parts of northern and central India, with most regions showing no change (figure 1C). The annual incidence of measles declines across almost all Indian states (except Rajasthan and Maharashtra), with Punjab, Uttarakhand, Madhya Pradesh, Chhattisgarh, Bihar, Odisha and Karnataka showing near-universal decline in districts within these states (figure 1D). Online supplemental appendix table A.1 shows the distribution of mean of change in VPD incidence per 1000 u5 children by 5-unit increments of their respective percentile distributions. We note that these distributions cohere with figure 1, in that the change in median annual incidence of DPT does not change between 2013 and 2016, but we observe a marginal decline in change in median annual incidence of measles (online supplemental appendix table A.1).
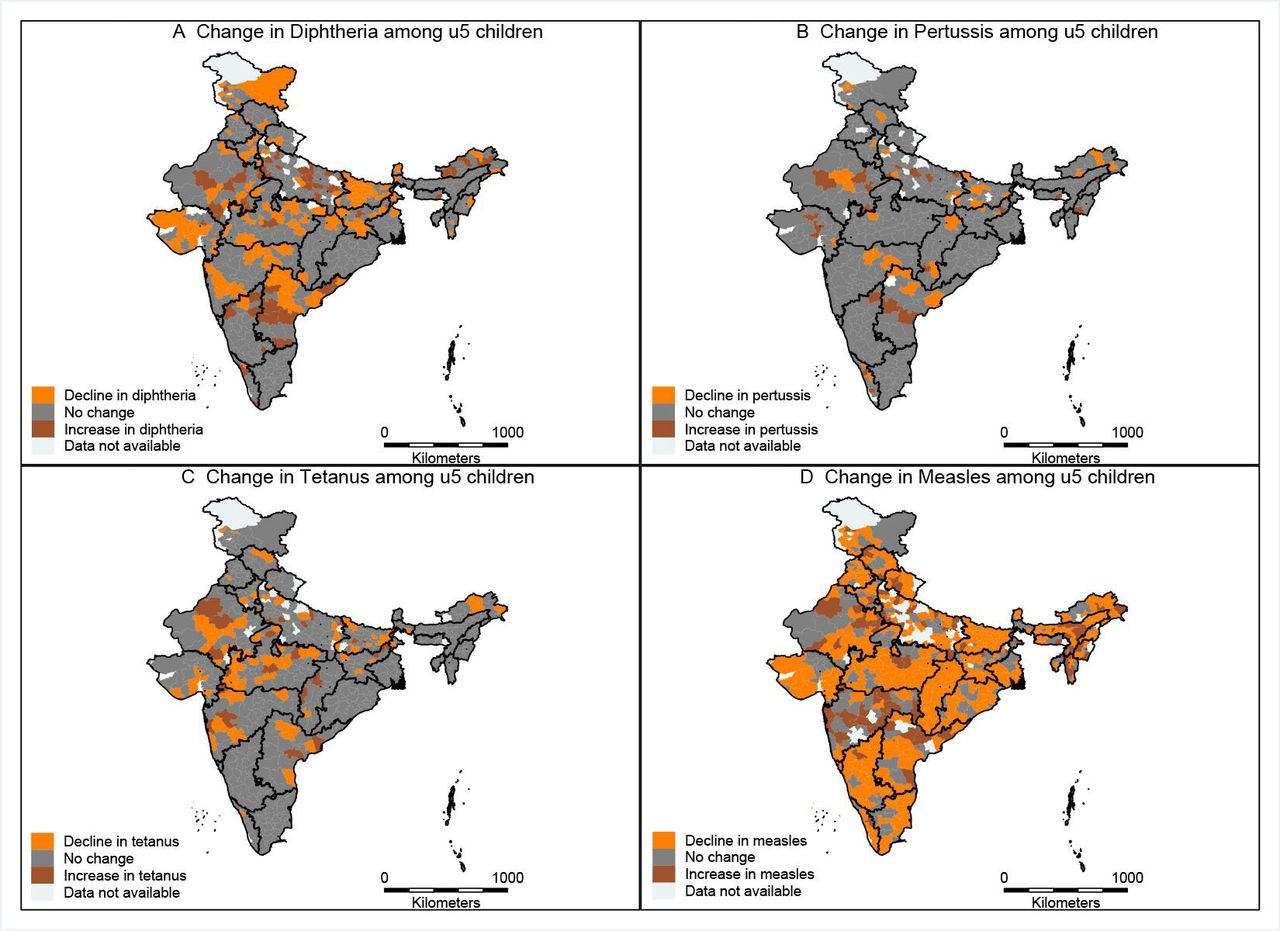
District-level maps of India showing change in diphtheria (A), pertussis (B), tetanus (C) and measles (D), from 2013 to 2016. Source: India shapefiles were obtained from publicly available GitHub repository: https://github.com/datameet/maps/find/master. Maps in manuscript have been created by authors.
Figure 2 maps the change in district-level percentage of households with toilets across India. We observe a near-uniform increase in household-level toilet availability nationwide.

{kind=link}
{kind=link}
District-level map of change in percentage of household with toilets in India (2013–2016). Source: India shapefiles were obtained from publicly available GitHub repository: https://github.com/datameet/maps/find/master. Maps in manuscript have been created by authors. SBM, Swachh Bharat Mission.
We observe no relation between increase in percentage of households with toilets and change in the annual incidence of DPT per 1000 u5 children (table 2, models 1–3). However, for every one per cent increase in exposure, the annual incidence of measles in u5 children (per 1000) declines by 0.33 units (coefficient=−0.33, 95% CI −0.641 to –0.014, p<0.05) (table 2, model 4). This inverse relation concentrates in central and north eastern Indian districts (online supplemental appendix table A.2), presumably owing to greater change in percentage of households with toilets in these two regions (online supplemental appendix table A.3). Examination of change in counts (rather than annual incidence per 1000 u5 children) of u5 measle cases indicates 0.16 fewer cases associated with every one percentage point increase in exposure. Put in another way, for a 7% increase in households with toilets (ie, mean change reported in table 1), our analyses suggest 1.12 fewer cases of measles in u5 children per district, on average, over our study period (online supplemental appendix figure A.1).
Linear regression predicting change in VPDs as a function of change in percentage of households with toilets, controlling for change in other covariates and baseline (pre-SBM) annual incidence of VPDs (N=532)
Vaccine response to measles relies on vitamin A supplementation and absorption.46 Vitamin A supplementation increased from 54% in 2013 to 71% in 2016 among u5 children in India.47 This increase, combined with increased toilet availability (and potential reduction in environmental enteropathy) in some districts, may correspond with improved absorption of Vitamin A in u5 children. We gauged whether and to what extent our results from table 2 (model 4) may be driven by changes in vitamin supplementation among u5 children. Online supplemental appendix table A.4 shows the results from inclusion of this variable as a covariate (all other specifications identical to table 2, model 4). A one unit increase in percentage of u5 children who received vitamin A supplementation is associated with a 0.19 percentage point decline in measles among u5 children (online supplemental appendix table A.4). Adjusting for this covariate marginally increases the association between change in toilet availability and change in measles among u5 children (relative to table 2, Model 4), indicating potential additive interaction with the main exposure.
As an exploratory exercise, we examined whether change in u5 child undernutrition—modelled as change in percentage of u5 children who are stunted—mediates the association between toilet availability and measles among u5 children in our analysis. We retrieved district-level data on u5 stunting from the NFHS, DLHS and AHS data sets (for details of this process, see Singh et al).30 We applied structural equation modelling techniques to examine direct, indirect and total effects of change in percentage of households with toilets on change in measles among u5 children, with change in u5 stunting specified as a mediator (online supplemental appendix table A.5).48 49 Results from this analysis indicate that about 12% of the total effect of change in percentage of households with toilets on change in measles among u5 children appears to be mediated by change in stunting among u5 children over our study period (online supplemental appendix table A.5).
We also examined whether our main results may be driven by outliers. We conducted two robustness checks wherein we (1) log-transformed the change in measles (outcome) to reduce the effect of potential outliers and re-estimated equation 1 (online supplemental appendix table A.6) and (2) z-scaled the outcome, removed observations beyond ±3 SD and re-estimated equation 1 (online supplemental appendix table 7). Results from these analyses (online supplemental appendix table A.6 and A.7) indicate that removal or adjustment of outliers does not alter our original inference.
Discussion
The SBM programme, launched in 2014 by the Government of India, aimed to eliminate open defecation through intensive behavioural change messaging and construction of over 100 million toilets nationwide.28 We examined whether and to what extent increase in toilet availability varied inversely with four VPDs (DPT and measles) in u5 children. We find that regional increases in percentage of households with toilets are associated with a small reduction in measles, but not in diphtheria, pertussis or tetanus. All results remain robust to several sensitivity analyses including control for outliers. We encourage replication of our findings as well as extensions on potential mechanistic pathways to determine whether improvements in ambient sanitation assist with reducing the burden of measles.
Strengths of this study include the utilisation of precise timing of an exogenously determined public sanitation programme (SBM), which establishes temporal order, minimises bias due to confounding and precludes the potential of reverse causation. The brief time lag post-SBM also minimises the risk of confounding due to the plausible rival of ‘maturation’, in which a variety of infrastructure improvements and cultural changes, which follow SBM but are not caused by SBM, improve child health overall. Maturation, for instance, would tend to threaten validity had we extended the time-horizon to several years post-intervention.50 In addition, we use large, nationally representative data sources that are publicly available. Finally, we account for baseline differences across districts in the annual incidence of VPDs, which reduces the threat of regression to the mean over the study period.
We offer two post hoc explanations for the disease-specific patterning of our results. First, the highly contagious nature of measles (relative to DPT) may impart greater amenability to change, following SBM. Second, diagnosis of measles often carries lower ambiguity (owing to distinct rash) relative to diphtheria or pertussis (which commonly present with cough and/or fever), which may correspond with underdiagnosis and under-reporting of the latter.51–53 This low reporting may have precluded us from detecting the ‘true magnitude of cases averted by SBM, even if a true relation between SBM and lower DPT cases actually occurred.
Other infectious diseases closely linked to transmission via the fecal-oral route include cholera, salmonella, hepatitis A and rotavirus, which account for a large majority of diarrheal episodes in India.54 Repeated diarrheal infections further exacerbate pre-existing environmental enteropathy, undernutrition and vaccine failure,5 8 whereas we do not know of any nationally representative, publicly available data sets that report annual district-level cholera, salmonella, hepatitis A and rotavirus surveillance in u5 children, we encourage policymakers to provide this information for future research and evaluation of sanitation improvements on these diseases.
Limitations
The non-controlled nature of the study (ie, the lack of a randomised controlled trial), as well as lack of mechanistic data on environmental enteropathy, indicates that our findings should be viewed as suggestive rather than definitive. Only replication and extension of our work could more firmly support a causal relation between the SBM campaign and reduced measles in u5 children. In addition, we could not analyse urban and rural regions separately because the HMIS data do not report annual incidence of VPD by rural/urban divisions within districts. Owing to data limitations, we also cannot examine differential responses by gender or age groups.30 Data limitations also did not permit a more nuanced spatial analysis that takes into consideration the similar of some adjacent districts (but not others) within a region with respect to sanitation and measle incidence. Furthermore, measle incidence may fall over time even absent SBM. To the extent that causes of such declines correlate with, but are not caused by, the region-level intensity of toilet construction, findings may have residual confounding. In addition, shared toilet use presents a key point of contamination and exposure to faecal matter. We do not examine networks of households that share toilets and their relation of VPDs among children in this study owing to lack of individual-level information in the HMIS data set. Future research may explore the role of shared toilet on child health if such data become available.
We did not have access to biological markers of environmental enteropathy, which may have offered clinically definitive methods to identify this condition as well as subsequent physiological changes following improved ambient sanitation.16 Intestinal biopsies conducted in the 1960s, such as those by Lindebaum and colleagues, may not serve as feasible means for identification of enteropathy in current epidemiological studies.27 Recent research identifies malabsorption, changes in local immune activity and intestinal permeability as key diagnostic features of environmental enteropathy.16 Measurement of biomarkers of carbohydrate malabsorption (eg, lactulose-mannitol), mucosal activity (eg, T-helper cell type 1), serum protein from intestinal mucosa and markers of systemic immune activity and inflammation (eg, C reactive protein, glycoproteins) may provide direct evidence of environmental enteropathy.16 Such analyses may augment ecological research in understanding clinical as well as epidemiological ramifications of improved sanitation on child health.
Conclusion
Findings, if replicated, indicate that improvements in ambient sanitation through construction and utilisation of toilets may augment current efforts in reducing the burden of VPDs among children in India.
Data availability statement
Data are available in a public, open access repository. The datasets underlying this article are available from the following sources in the public domain: 1. Health Management Information System (HMIS) India: Health Management Information System: A digital initiative under National Health Mission. Ministry of Health & Family Welfare, Government of India. 2020. Available from: https://dhsprogram.com/pubs/pdf/FR339/FR339.pdf 2. Annual Health Survey (second round): Annual Health Survey (AHS) India. Office of the Registrar General and Census Commissioner (India) 2014. URL: http://www.censusindia.gov.in/2011census/hh-series/cab.html 3. District Level Household and Facility Survey (DLHS-4), 2012–13. IIPS, International Institute of Population Sciences, Mumbai, India. Deonar, Mumbai, 2014. URL: http://www.nrhmmis.nic.in/SitePages/DLHS-4.aspx 4. National Family Health Survey (NFHS-4): International Institute for Population Sciences (IIPS) and ICF. National Family Health Survey (NFHS-4), 2015-16: India. Mumbai: IIPS 2017. URL: https://dhsprogram.com/pubs/pdf/FR339/FR339.pdf.
Ethics statements
Patient consent for publication
Ethics approval
This study used publicly available, deidentified secondary data and was IRB exempt per rules specified by the University of California Irvine.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors PS: conceptualisation; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; validation; visualisation; roles/writing—original draft; writing—review and editing. DNF: conceptualisation; investigation; supervision; validation; roles/writing—original draft; writing—review and editing. MS: formal analysis; investigation; methodology; supervision; validation; roles/writing—original draft; writing—review and editing. T-AB: conceptualisation; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; validation; visualisation; roles/writing—original draft; writing—review and editing. PS is the guarantor.
Funding Funding for this research was provided by the National Institute of Allergy and Infectious Diseases: 1R03AI135322-01.
Disclaimer The funding source had to involvement in in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct and dissemination of this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.