Reader Comments
Post a new comment on this article
Post Your Discussion Comment
Please follow our guidelines for comments and review our competing interests policy. Comments that do not conform to our guidelines will be promptly removed and the user account disabled. The following must be avoided:
- Remarks that could be interpreted as allegations of misconduct
- Unsupported assertions or statements
- Inflammatory or insulting language
Thank You!
Thank you for taking the time to flag this posting; we review flagged postings on a regular basis.
closeEstrogen is associated with greater suicidality among transgender males, and puberty suppression is not associated with better mental health outcomes for either sex
Posted by MichaelBiggs on 19 Jan 2022 at 03:19 GMT
Using a large online survey of Americans who identified as transgender, nonbinary, or cross-dressers, Turban et al. [1] find that 'people who accessed GAH [cross-sex hormones] during early or late adolescence had a lower odds of past-month suicidal ideation and past-month severe psychological distress in adulthood, when compared to those who desired but did not access GAH [cross-sex hormones], after adjusting for a range of potential confounding variables.' They also find that respondents who started these hormones as adults had higher odds of binge drinking and of illegal drug use--though this finding does not appear in the abstract, introduction or conclusion. This article is the latest to mine the United States Transgender Survey (USTS) [2-7]. This data source has serious deficiencies [8,9]. The survey was not representative of the transgender population. In addition, the survey excluded individuals who no longer identified as transgender, the group most likely to be harmed by cross-sex hormones [10,11]. Although cross-sex hormones are supposed to be a treatment for 'persistent, well-documented gender dysphoria,' the survey asked no questions about gender dysphoria [12]. Finally, the data are retrospective, and so any positive association between mental health and endocrinological interventions could simply indicate that clinicians were reluctant to prescribe those interventions for patients with poor mental health. After all, the World Professional Association for Transgender Health's Standards of Care states that a prerequisite for prescribing cross-sex hormones is that 'significant medical or mental health concerns ... must be reasonably well-controlled' [12].
Turban et al.'s article raises three questions. The first is why 'the range of confounding variables' omits interventions which have been identified in other published studies using the same data--including those with shared authors--as having positive associations with the same outcomes. According to Almazan and Keuroglian, for example, respondents who had undergone surgeries like double mastectomy and vaginoplasty reported better mental health [7]. Why, then, is this variable omitted by Turban et al.? Conversely, a previous article by Turban et al. claimed to find a positive association between puberty suppression (using a Gonadotropin-Releasing Hormone agonist) and mental health--but this did not control for cross-sex hormones [5]. The current article includes pubertal suppression as a confounding variable, but omits to report the result. I will report that it has no statistically significant effect on mental health, which refutes their earlier finding.
The second question is why the effect of estrogen on males is assumed to be identical to the effect of testosterone on females. Testing this assumption, I will demonstrate that the associations differ significantly in magnitude--and for some outcomes, the direction of the association diverges. Males who took estrogen are more likely to plan suicide, to attempt suicide, and to require hospitalization for a suicide attempt. The third question is posed by the authors' analytical strategy of restricting the control group to respondents who wanted cross-sex hormones. Why not also compare respondents who did not want such hormones? I will demonstrate that not wanting cross-sex hormones is associated with better outcomes for males than taking estrogen.
METHODS
Turban et al. analyze several binary outcomes. One is extreme psychological distress in the past month (13 or more on the Kessler-6 scale), which is a proxy for severe mental illness. Another is suicidality in the past 12 months, measured by a sequence of questions, starting with 'did you seriously think about trying to kill yourself?' and ending with 'Did you stay in a hospital overnight or longer because you tried to kill yourself?' These responses are treated as separate binary variables. (The responses should be treated as a single ordinal variable, but my analysis follows the authors' method.) The final pair of outcomes are binge drinking and illicit drug use. These are not analyzed here because Turban et al.'s findings for these outcomes undermine their own argument.
Turban et al. initially define three treatment groups according to the age at which cross-sex hormones commenced: 14 or 15; 16 or 17; 18 and over. They find no statistically significant difference between the two younger groups and so I combine them. Their control group comprises respondents who wanted cross-sex hormones but had never obtained them. I will also compare another control group, respondents who did not want cross-sex hormones. The authors select different subsets of control variables in each statistical model, drawing from the following: sex, race, age, education, employment status, household income, sexual orientation, gender identity (transgender, nonbinary, or cross-dresser), support from family, relationship status, experiencing harassment for being transgender at school, and having a professional 'try to stop you being trans.' I will consistently use all these control variables in each model.
Turban et al.'s analysis is impossible to replicate exactly because they do not provide sufficient details of their coding and analysis. For example, they do not state whether they use sampling weights. (The authors have twice previously not replied to my requests to provide their command files.) My analysis uses the 'standard survey weight' provided by USTS, which rebalances the suspiciously large number of respondents who claimed to be 18 years of age and the overrepresentation of whites. There are odd discrepancies between the raw frequencies reported by Turban et al. and the USTS dataset. According to the authors, 119 respondents reported beginning cross-sex hormones at age 14 or 15. But for the question 'At what age did you begin hormone treatment' (Q12.10), 27 respondents answered at age 14, and 61 answered at age 15, summing to 88. How did the authors obtain an additional 31 observations? It is not due to the imputation of missing values because the authors drop observations with missing values; the same procedure is followed here.
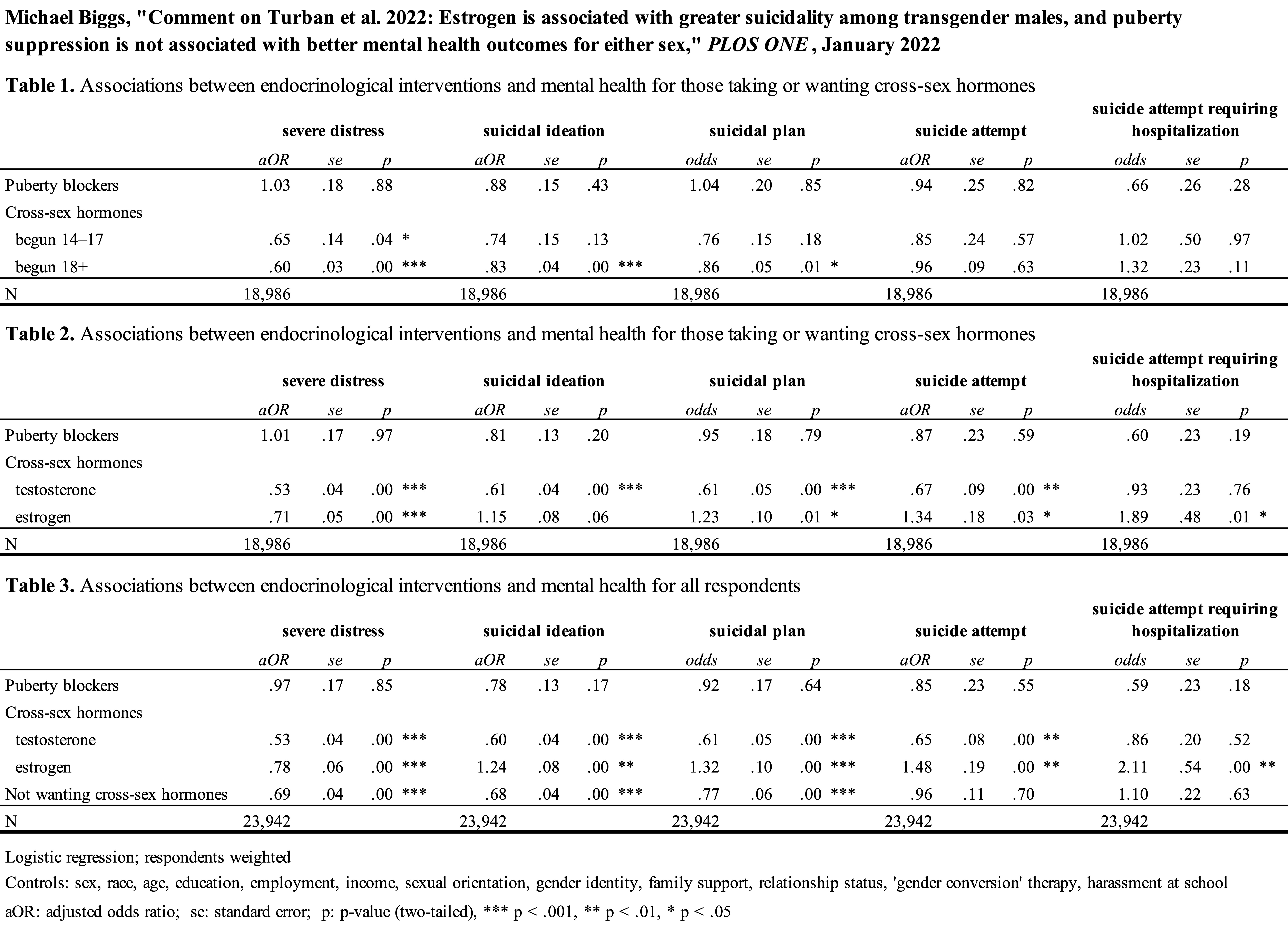
RESULTS [tables at https://users.ox.ac.uk/~s...]
Using the sample defined by Turban et al., Table 1 compares 381 respondents who had started cross-sex hormones in adolescence and 11,137 who had started in adulthood with 7,468 who wanted these hormones but had never used them. Differences between age groups are minimal and are not statistically significant (testing differences between coefficients, p = .55 ... .73), which is not surprising seeing that relatively few commenced cross-sex hormones under the age of 18. Controlling for the other variables, respondents taking cross-sex hormones are significantly less likely to suffer severe distress and to entertain suicidal thoughts than respondents who wanted them. These results therefore replicate Turban et al.'s headline results. Furthermore, respondents who commenced cross-sex hormones in adulthood are less likely to plan suicide. Besides cross-sex hormones, the other endocrinological intervention is puberty suppression. Controlling for other variables, having taken puberty blockers has no statistically significant association with any outcome. This reveals that Turban et al.'s earlier finding from the USTS--which did not control for cross-sex hormones--is not robust [5].
Table 2 tests the authors' assumption that testosterone for females is the same as estrogen for males. (The effect of puberty suppression does not differ by sex.) The assumption is falsified. After controlling for other variables, every outcome's association with testosterone differs significantly from its association with estrogen (testing differences between coefficients, p = .004 for severe distress, p = .035 for suicide attempt requiring hospitalization, and p < .001 for other outcomes). Testosterone is consistently associated with better outcomes. Estrogen is associated with a lower probability of severe distress, but also with a higher probability of planning, attempting, and being hospitalized for suicide. The latter outcome is particularly disturbing: males who took estrogen have almost double the adjusted odds of a suicide attempt requiring hospitalization.
Table 3 adds respondents who did not want (and had not taken) cross-sex hormones as a separate control group, numbering 4,956. Compared to respondents who wanted but had not obtained cross-sex hormones, and adjusting for other variables, these respondents are less likely to suffer severe distress, less likely to have suicidal thoughts, and less likely to plan suicide. The comparison between these respondents and the respondents taking cross-sex hormones differs by sex. For females, those who took testosterone are less likely to be severely distressed and to plan and attempt suicide than those who did not want testosterone (testing differences between coefficients, p = .002, p = .02, and p = .02 respectively). For males, however, those who took estrogen are more likely to be suicidal than those who did not want estrogen (testing differences between coefficients, p < .001 for ideation, p < .001 for planning, p = .004 for attempting, and p = .02 for hospitalization).
CONCLUSION
Reanalysis of the data used by Turban et al. corrects their claims about the association between cross-sex hormones and mental health. Most importantly, the association differed according to sex. Controlling for other variables, females who took testosterone reported better outcomes than females who had not taken it, including those who did not even want it. Perhaps this is unsurprising given that several randomized control trials find testosterone acting as an anti-depressant [13]. In stark contrast, however, males taking estrogen reported greater suicidality than males not taking estrogen.
Secondly, the association between cross-sex hormones and mental health depends on the choice of comparison group. Take severe distress as an example. Compared to males who wanted estrogen but did not access it, males who took the hormone were less likely to have suffered severe distress; this accords with Turban et al.'s conclusions. But males who did not want cross-sex hormones were even less likely to have suffered severe distress. If one follows the authors in inferring causation from cross-sectional association, then one must conclude that not wanting this treatment improves males' mental health. The paradox could be resolved as follows: desire for estrogen is a proxy for pronounced gender dysphoria; estrogen helps transgender males with such pronounced gender dysphoria by reducing their chance of severe distress, albeit not to the low level enjoyed by transgender males who have less dysphoria. This resolution is purely conjectural, however, because USTS did not measure gender dysphoria. The nearest was a question on gender identity, which is already included as a control variable.
In conclusion, then, Turban et al.'s finding that access to cross-sex hormones 'during adolescence and adulthood is associated with favorable mental health outcomes compared to desiring but not accessing' such hormones can be extracted from the USTS only by denying the difference between testosterone and estrogen. The authors' recommendation 'that these medical interventions be made available for transgender adolescents' has no justification. Perhaps one could claim that the survey provides some evidence that testosterone reduces distress and suicidality in females. But then one must also admit that it also provides evidence that estrogen increases suicidality in males and that puberty blockers offer no benefit. It is not legitimate to pick out the results ostensibly favoring medical intervention while ignoring equally credible evidence for its detrimental effects. The real question is why the authors return again and again to this online survey--which did not even measure the condition supposed to be treated, namely gender dysphoria--rather than conducting randomized control trials or collecting longitudinal patient data.
REFERENCES
1. Turban JL, King D, Kobe J, Reisner SL, Keuroghlian AS. Access to gender-affirming hormones during adolescence and mental health outcomes among transgender adults. PLOS ONE. 2022;17: e0261039. doi:10.1371/journal.pone.0261039
2. Lelutiu-Weinberger C, English D, Sandanapitchai P. The roles of gender affirmation and discrimination in the resilience of transgender individuals in the US. Behav Med. 2020;46: 175-188. doi:10.1080/08964289.2020.1725414
3. Scheim AI, Perez-Brumer AG, Bauer GR. Gender-concordant identity documents and mental health among transgender adults in the USA: a cross-sectional study. Lancet Public Health. 2020;5: e196-e203. doi:10.1016/S2468-2667(20)30032-3
4. Turban JL, Beckwith N, Reisner SL, Keuroghlian AS. Association between recalled exposure to gender identity conversion efforts and psychological distress and suicide attempts among transgender adults. JAMA Psychiatry. 2020;77: 68-76. doi:10.1001/jamapsychiatry.2019.2285
5. Turban JL, King D, Carswell JM, Keuroghlian AS. Pubertal suppression for transgender youth and risk of suicidal ideation. Pediatrics. 2020;145: e20191725. doi:10.1542/peds.2019-1725
6. Yockey A, King K, Vidourek R. Past-year suicidal ideation among transgender individuals in the United States. Arch Suicide Res. 2020. doi:10.1080/13811118.2020.1803165
7. Almazan AN, Keuroghlian AS. Association between gender-affirming surgeries and mental health outcomes. JAMA Surg. 2021. doi:10.1001/jamasurg.2021.0952
8. Biggs M. Puberty blockers and suicidality in adolescents suffering from gender dysphoria. Arch Sex Behav. 2020;49: 2227-2229. doi:10.1007/s10508-020-01743-6
9. D'Angelo R, Syrulnik E, Ayad S, Marchiano L, Kenny DT, Clarke P. One size does not fit all: In support of psychotherapy for gender dysphoria [Letter to the Editor]. Arch Sex Behav. 2021;50: 7-16. doi:10.1007/s10508-020-01844-2
10. Littman L. Individuals treated for gender dysphoria with medical and/or surgical transition who subsequently detransitioned: A survey of 100 detransitioners. Arch Sex Behav. 2021. doi:10.1007/s10508-021-02163-w
11. Vandenbussche E. Detransition-related needs and support: A cross-sectional online survey. J Homosex. 2021. doi:10.1080/00918369.2021.1919479
12. Coleman E, Bockting W, Botzer M, Cohen-Kettenis P, DeCuypere G, Feldman J, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people, version 7. Int J Transgenderism. 2012;13: 165-232. doi:10.1080/15532739.2011.700873
13. Walther A, Breidenstein J, Miller R. Association of testosterone treatment with alleviation of depressive symptoms in men: a systematic review and meta-analysis. JAMA Psychiatry. 2019;76: 31-40. doi:10.1001/jamapsychiatry.2018.2734
RE: Estrogen is associated with greater suicidality among transgender males, and puberty suppression is not associated with better mental health outcomes for either sex
DrRow replied to MichaelBiggs on 08 Mar 2022 at 13:26 GMT
Thank you for providing this additional information regarding the data set and this study. We must not ignore data that does not fit the narrative, but rather change the narrative to fit the data.

{kind=link}